Knee Arthroscopy
If you have persistent pain, catching, or swelling in your knee, a procedure known as arthroscopy may help relieve these problems.
Arthroscopy allows an orthopaedic surgeon to diagnose and treat knee disorders by providing a clear view of the inside of the knee with small incisions, utilizing a pencil-sized instrument called an arthroscope. The scope contains optic fibers that transmit an image of your knee through a small camera to a television monitor. The TV image allows the surgeon to thoroughly examine the interior of your knee and determine the source of your problem. During the procedure, the surgeon also can insert surgical instruments through other small incisions in your knee to remove or repair damaged tissues.
Modern or contemporary arthroscopy of the knee was first performed in the late 1960s. With improvements of arthroscopes and higher-resolution cameras, the procedure has become highly effective for both the accurate diagnosis and proper treatment of knee problems. Today, arthroscopy is one of the most common orthopaedic procedures in the United States.
Whether you have just begun exploring treatment options for your problem knee or have already decided, with your orthopaedic surgeon, to have an arthroscopy, this booklet will help you understand more about this valuable procedure.
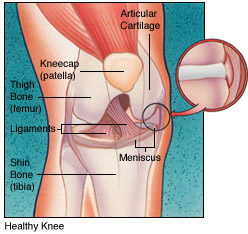
How the Normal Knee Works
The knee is the largest joint in the body, and one of the most easily injured. It is made up of the lower end of the thigh bone (femur), the upper end of the shin bone (tibia), and the knee cap (patella), which slides in a groove on the end of the femur. Four bands of tissue, the anterior and posterior cruciate ligaments, and the medial and lateral collateral ligaments connect the femur and the tibia and provide joint stability. Strong thigh muscles give the knee strength and mobility.
The surfaces where the femur, tibia and patella touch are covered with articular cartilage, a smooth substance that cushions the bones and enables them to glide freely. Semicircular rings of tough fibrous-cartilage tissue called the lateral and medial menisci act as shock absorbers and stabilizers.
The bones of the knee are surrounded by a thin, smooth tissue capsule lined by a thin synovial membrane which releases a special fluid that lubricates the knee, reducing friction to nearly zero in a healthy knee.
Knee Problems
Normally, all parts of the knee work together in harmony. But sports, work injuries, arthritis, or weakening of the tissues with age can cause wear and inflammation, resulting in pain and diminished knee function.
Arthroscopy can be used to diagnose and treat many of these problems:

- Torn meniscal cartilage.
- Loose fragments of bone or cartilage.
- Damaged joint surfaces or softening of the articular cartilage known as chondromalacia.
- Inflammation of the synovial membrane, such as rheumatoid or gouty arthritis.
- Abnormal alignment or instability of the kneecap.
- Torn ligaments including the anterior and posterior cruciate ligaments.
 |
By providing a clear picture of the knee, arthroscopy can also help the orthopaedic surgeon decide whether other types of reconstructive surgery would be beneficial.
|
Is Arthroscopy for You? 
Your family physician can refer you to an orthopaedic surgeon for an evaluation to determine whether you could benefit from arthroscopy.
Signs that you may be a candidate for this procedure include swelling, persistent pain, catching, giving-way, and loss of confidence in your knee. When other treatments such as the regular use of medications, knee supports, and physical therapy have provided minimal or no improvement, you may benefit from arthroscopy.
Most arthroscopies are performed on patients between the ages of 20 and 60, but patients younger than 10 years and older than 80 years have benefited from the procedure.
The Orthopaedic Knee Evaluation 
- A medical history, in which your orthopaedic surgeon gathers information about your general health and asks you about your symptoms.
- A physical examination to assess your knee motion and stability, muscle strength and overall leg alignment.
- X-rays to evaluate the bones of your knee. Your orthopaedic surgeon may also arrange for you to have an MRI to provide more information about the soft tissues of your knee. An MRI uses magnetic sound waves to create images. They are not X-rays. Blood tests may be obtained to determine if you have arthritis.
Your orthopaedic surgeon will review the results of your evaluation with you and discuss whether arthroscopy would be the best method to further diagnose and treat your knee problem. Other treatment options, such as medications or other surgical procedures also will be discussed and considered.
Your orthopaedic surgeon will explain the potential risks and complications of knee arthroscopy, including those related to the surgery itself and those that can occur after your surgery.
Preparing for Surgery
If you decide to have arthroscopy, you may be asked to have a complete physical with your family physician before surgery to assess your health and to rule out any conditions that could interfere with your surgery.
Before surgery, tell your orthopaedic surgeon about any medications that you are taking. You will be informed which medications you should stop taking before surgery.
Tests, such as blood samples or a cardiogram, may be ordered by your orthopaedic surgeon to help plan your procedure.
Your Arthroscopic Knee Surgery
Almost all arthroscopic knee surgery is done on an outpatient basis. Your hospital or surgery center will contact you about the specific details for your surgery, but usually you will be asked to arrive at the hospital an hour or two prior to your surgery. Do not eat or drink anything after midnight the night before your surgery.
After arrival, you will be evaluated by a member of the anesthesia team. Arthroscopy can be performed under local, regional, or general anesthesia. Local anesthesia numbs your knee, regional anesthesia numbs you below your waist, and general anesthesia puts you to sleep. The anesthesiologist will help you determine which would be the best for you.
 If you have local or regional anesthesia, you may be able to watch the procedure on a TV screen, if you wish.
If you have local or regional anesthesia, you may be able to watch the procedure on a TV screen, if you wish.
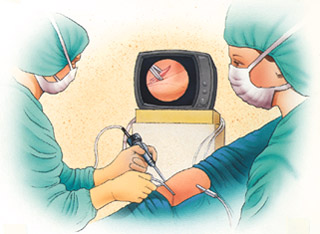
The orthopaedic surgeon will make a few small incisions in your knee. A sterile solution will be used to fill the knee joint and rinse away any cloudy fluid, providing a clear view of your knee.
The surgeon will then insert the arthroscope to properly diagnose your problem, using the TV image to guide the arthroscope. If surgical treatment is needed, the surgeon can use a variety of small surgical instruments (e.g., scissors, clamps, motorized shavers, or lasers) through another small incision. This part of the procedure usually lasts 45 minutes to 1 1/2 hours.
Common treatments with knee arthroscopy include:
- Removal or repair of torn meniscal cartilage.
- Reconstruction of a torn cruciate ligament.
- Trimming of torn pieces of articular cartilage.
- Removal of loose fragments of bone or cartilage.
- Removal of inflamed synovial tissue.
At the conclusion of your surgery, the surgeon may close your incisions with a suture or paper tape and cover them with a bandage.
You will be moved to the recovery room. Usually, you will be ready to go home in one or two hours. You should have someone with you to drive you home.
Your Recovery at Home
 Recovery from knee arthroscopy is much faster than recovery from traditional open knee surgery. Still, it is important to follow your orthopaedic surgeon's instructions carefully after you return home. You should ask someone to check on you that evening.
Recovery from knee arthroscopy is much faster than recovery from traditional open knee surgery. Still, it is important to follow your orthopaedic surgeon's instructions carefully after you return home. You should ask someone to check on you that evening.
Swelling Keep your leg elevated as much as possible for the first few days after surgery. Apply ice as recommended by your orthopaedic surgeon to relieve swelling and pain.
Dressing Care You will leave the hospital with a dressing covering your knee. You may remove the dressing the day after surgery. You may shower, but should avoid directing water at the incisions. Do not soak in a tub. Keep your incisions clean and dry.
Your orthopaedic surgeon will see you in the office a few days after surgery to check your progress, review the surgical findings, and begin your postoperative treatment program.
Bearing Weight After most arthroscopic surgeries, you can walk unassisted but your orthopaedic surgeon may advise you to use crutches, a cane, or a walker for a period of time after surgery. You can gradually put more weight on your leg as your discomfort subsides and you regain strength in your knee. Your surgeon may allow you to drive after a week.
 Exercises to Strengthen Your Knee You should exercise your knee
Exercises to Strengthen Your Knee You should exercise your knee
regularly for several weeks following surgery to strengthen the muscles of
your leg and knee. A physical therapist may help you with your exercise
program if your orthopaedic surgeon recommends specific exercises.
Medications Your orthopaedic surgeon may prescribe antibiotics to help prevent an infection and pain medication to help relieve discomfort following your surgery.
Complications Potential postoperative problems with knee arthroscopy include infection, blood clots, and an accumulation of blood in the knee. These occur infrequently and are minor and treatable.
Warning Signs
Call your orthopaedic surgeon immediately if you experience any of the following:
- Fever.
- Chills.
- Persistent warmth or redness around the knee.
- Persistent or increased pain.
- Significant swelling in your knee.
- Increasing pain in your calf muscle.
- Shortness of breath or chest pain.
Reasonable Expectations After Arthroscopic Surgery
 Although arthroscopy can be used to treat many problems, you may have some activity limitations even after recovery. The outcome of your surgery will often be determined by the degree of injury or damage found in your knee. For example, if you damage your knee from jogging and the smooth articular cushion of the weight-bearing portion of the knee has worn away completely, then full recovery may not be possible. You may be advised to find a low-impact alternative form of exercise. An intercollegiate or professional athlete often sustains the same injury as a weekend recreational athlete, but the potential for recovery may be improved by the over-development of knee muscles. Physical exercise and rehabilitation will play an important role in your final outcome. A formal physical therapy program also may add something to your final result.
Although arthroscopy can be used to treat many problems, you may have some activity limitations even after recovery. The outcome of your surgery will often be determined by the degree of injury or damage found in your knee. For example, if you damage your knee from jogging and the smooth articular cushion of the weight-bearing portion of the knee has worn away completely, then full recovery may not be possible. You may be advised to find a low-impact alternative form of exercise. An intercollegiate or professional athlete often sustains the same injury as a weekend recreational athlete, but the potential for recovery may be improved by the over-development of knee muscles. Physical exercise and rehabilitation will play an important role in your final outcome. A formal physical therapy program also may add something to your final result.
A return to intense physical activity should only be done under the direction of your surgeon.
It is reasonable to expect that by six to eight weeks you should be able to engage in most of your former physical activities as long as they do not involve significant weight-bearing impact. Twisting maneuvers may have to be avoided for a longer time.
If your job involves heavy work, such as a construction laborer, you may require more time to return to your job than if you have a sedentary job.
Your orthopaedic surgeon is a medical doctor with extensive training in the diagnosis and nonsurgical and surgical treatment of the musculoskeletal system, including bones, joints, ligaments, tendons, muscles, and nerves.
This brochure has been prepared by the American Academy of Orthopaedic Surgeons and is intended to contain current information on the subject from recognized authorities. However, it does not represent official policy of the Academy and its text should not be construed as excluding other acceptable viewpoints. Persons with questions about a medical condition should consult a physician who is informed about the condition and the various modes of treatment available.
Reviewed 2000
All Information Copyright © American Academy of Orthopaedic Surgeons
www.aaos.org